

 I think I may have buried the lead in the last blog post. Perhaps this imaginary conversation will clarify what is so important about the George et al study.
I think I may have buried the lead in the last blog post. Perhaps this imaginary conversation will clarify what is so important about the George et al study.
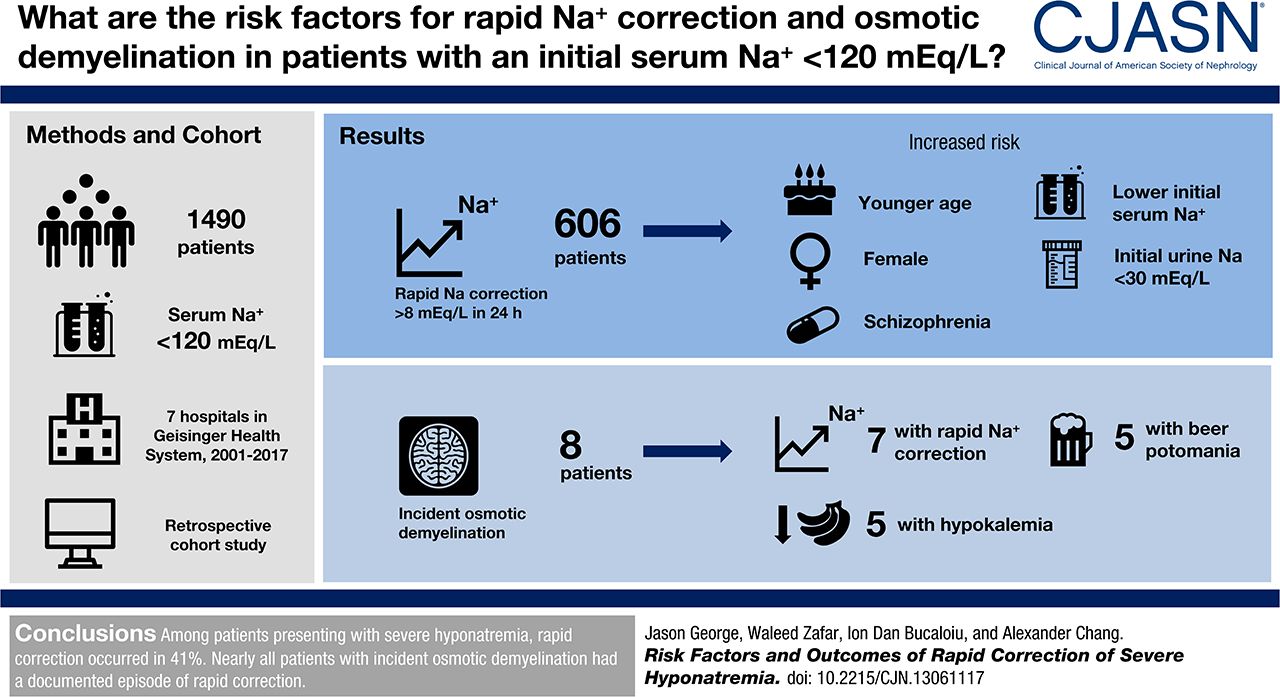
Nephrologist: There are now clinical practice guidelines, based on expert opinion, that tell us to correct sodium no more than 8 mmol/L in the first day of hyponatremia.
Internist: That seems cautious. How well are we meeting those guidelines?
Nephrologist: Well in a recent multi-center, retrospective analysis, of nearly 1500 people with an initial sodium below 120, just over 40% went too fast.
Internist: FORTY PERCENT were too fast. Oh my god! We’re doing horrible!
Nephrologist: Yeah, it’s kind of embarrassing.
Internist: So what happened to the 600+ people where the speed limit was exceeded?
Nephrologist: Well, they found 9 people had osmotic demyelination on MRI. But none of them had any documented permanent neurologic deficits and none of them was diagnosed with central pontine myelinolysis.
Internist: So how many people could we help if we worked on protocols, education and training to get that 40% closer to 5 or 10%?
Nephrologist: Well, since with a 40% miss rate we couldn’t find any harm, I guess we couldn’t expect much improvement with a 5 to 10% miss rate.
Internist: We should probably put our energy elsewhere.