


Renal stents for preservation of renal function with atherosclerotic renal artery stenosis
The annals has an article this week on renal stents and again they fail.
 Stent Placement in Patients With Atherosclerotic Renal Artery Stenosis and Impaired Renal Function
Stent Placement in Patients With Atherosclerotic Renal Artery Stenosis and Impaired Renal Function

They randomized 140 patients with GFR <>50% stenosis (CT angio, MRA or digital subtraction angiography) with in 1 cm of the origin of the renal artery. They also excluded patients with uncontrolled blood pressure (>140/90) this was done because if patients randomized to medical management developed uncontrollable blood pressure they could cross over and receive a stent.
The end point was a persistant 20% reduction of GFR by Cockcroft-Gault for more than a month.
Results: No significant difference between the two treatment strategies.
The Kaplan-Meier curves confirm this. The top graph is the primary outcome and the bottom graph is primary outcome plus death: Renal angioplasty resulted a variety of complications:
Renal angioplasty resulted a variety of complications:
Two patients in the stent group died of procedure-related causes within 30 days after stent placement. In 1 of the patients, embolization of a perforated renal artery was required; the patient subsequently developed pulmonary edema and needed mechanical ventilation, and died of a massive ischemic stroke 3 days later. The second patient had perforation of a renal artery branch; the artery was embolized, but despite re-intervention, the patient went into hypovolemic shock and experienced the acute respiratory distress syndrome, and died of multiorgan failure after 1 week.
The most common complications after stent placement were minor and mainly consisted of hematoma at the puncture site (11 patients [17%]). In 1 of these patients, secondary infection in the groin required surgical reconstruction. The patient thereafter developed end-stage renal failure, pulmonary edema, and heart failure and died 6 months after the procedure. In 2 other patients, stent placement was complicated by false aneurysm of the femoral artery. Injury to the kidney or renal artery occurred in 5 patients; however, this was never associated with loss of renal function and additional intervention was never required.
One patient in the stent group who had repeated angiography required permanent dialysis after cholesterol embolism.
So another negative trial of renal artery revascularization. We are still waiting for the publication of ASTRAL, a much larger and more definitive trial. CORAL is another trial which is ongoing and will shed further light on this subject.
Will the UK courts squash scientific discourse?
 This article about Simon Singh‘s battle with the British Chiropractic Association is frightening.
This article about Simon Singh‘s battle with the British Chiropractic Association is frightening.
The consequences of letting the libel law loose on scientific debate are horrendous. Science proceeds by peer review. A researcher’s colleagues must submit his or her ideas to scrutiny without fear of the consequences. If they think they could lose their homes and savings in the libel courts, however, they will back off.
For alternative therapists are not the only ones answering their critics with lawyers. NMT, an American health giant, is suing a British doctor for questioning one of its treatments.
Incredibly the BCA has won the first legal round.
The BCA sued for libel. And on May 7th Sir David Eady, a high-court judge, ruled, in a preliminary hearing, that the “natural and ordinary meaning” of the phrase (the relevant legal test) was that the BCA was being consciously dishonest and knowingly promoting quack treatments.
 The key to the court case is a claim that chiropractic treatments for problems outside of backpain are bogus that Singh made in Trick or Treatment: The Undeniable Facts about Alternative Medicine
The key to the court case is a claim that chiropractic treatments for problems outside of backpain are bogus that Singh made in Trick or Treatment: The Undeniable Facts about Alternative Medicine, a book he coauthored on alternative medicine.
Advancing medicine and science is impossible if writers have to self-censor themselves when discussing scientific claims.
UpToDate evidence based medicine or not? Not.
A few months ago medical blogger Laika wrote an insightful blog entry summarizing a meme which had been bouncing around twitter regarding whether UpToDate was evidence based medicine or some other entity.
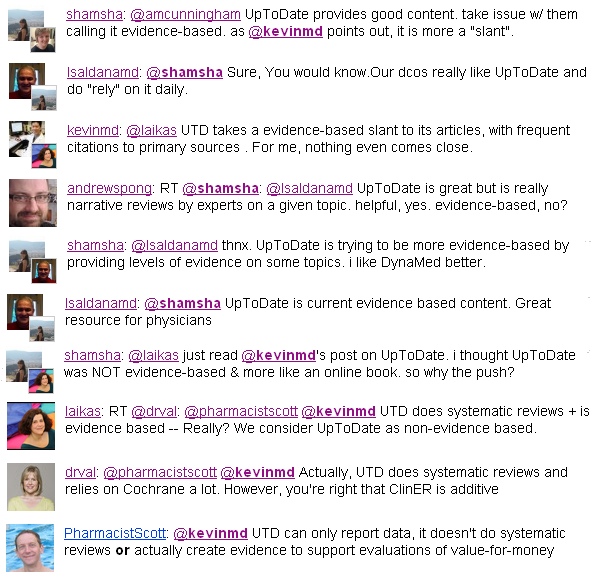
I found the whole excercise to be a bit too philosophical for me. Regardless of what you call it I think everyone would agree that UpToDate is useful. It is a great starting place but usually insufficient as a single source.
I was reminded about it today when I came across this paragraph:
 In the card on “Clinical manifestations, diagnosis, and natural history of primary biliary cirrhosis.” (Link for subsribers)
In the card on “Clinical manifestations, diagnosis, and natural history of primary biliary cirrhosis.” (Link for subsribers)
Regardless of the merits of UpToDate, nothing breaks the illussion of evidence based medicine like an author throwing out a random statistic like “approximately 15% of the 1,200 patients who I have seen…” without a reference. This is the epitome of expert oriented experiential medicine and has no place in EBM.
Journal Club: ECLIPSE Trial and Membranous Lupus
Clevipidine
Aronson et al. The ECLIPSE trials: comparative studies of clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for acute hypertension treatment in cardiac surgery patients. Anesth Analg (2008) vol. 107 (4) pp. 1110-21
Clevipidine is a short-acting, IV, calcium channel blocker licensed for blood pressure control. The ECLIPSE Trial is a randomized, multi-center, open-label, prospective trial of perioperative blood pressure control for cardiac surgery. clevidipine was compared to nitroglycerine, sodium-nitroprusside and nicardipine in three parallel trials. The primary outcome was safety with a secondary outcome of efficacy.
Efficacy was measured by a method I have never seen before. The key measure of efficacy was keeping the blood pressure in the normal range so the authors measured the area under the curve for time versus SBP outside of the target blood pressure:
 The authors found no difference in safety among the four drugs, though there was a pesky P=0.04 for increased death with sodium nitroprusside compared to clevidipine:
The authors found no difference in safety among the four drugs, though there was a pesky P=0.04 for increased death with sodium nitroprusside compared to clevidipine:
 Clevidipine was significantly more efficacious than all competitors as individuals (except nicardipine) and when compared to all comparators.
Clevidipine was significantly more efficacious than all competitors as individuals (except nicardipine) and when compared to all comparators.
 Lupus Membranous Nephritis
Lupus Membranous Nephritis
Austin et al. Randomized, controlled trial of prednisone, cyclophosphamide, and cyclosporine in lupus membranous nephropathy. J Am Soc Nephrol (2009) vol. 20 (4) pp. 901-11
Prospective randomized controlled trial to compared cyclosporin for 11 months, to alternate-month cyclophosphamide for 11 months, to alternate-day prednisone alone.
Primary outcome was time to remission (less than 0.3 g of protein). Both CSA and prednisone were significantly better at achieving remission (complete and partial) than oral prednisone:
Both CSA and prednisone were significantly better at achieving remission (complete and partial) than oral prednisone: As we have seen in prior trials of cyclosporin in proteinuric renal disease (see FSGS), when the cyclosporin is stopped the proteinuria returns:
As we have seen in prior trials of cyclosporin in proteinuric renal disease (see FSGS), when the cyclosporin is stopped the proteinuria returns: A well done, but small trial. Good to see an RCT in this rare entity because evidence based data on how to handle membranous lupus has been scant.
A well done, but small trial. Good to see an RCT in this rare entity because evidence based data on how to handle membranous lupus has been scant.
What’s new in Potassium: sudden cardiac death
As the Nephrology Fellow Network recently covered the etiology of cardiovascular disease in dialyzors is unique from the general public. Use of statins, the foundation of preventative cardiology, has repeatedly failed to prevent cardiovascular vascular disease (CVD) among dialyzors. One reason for this, is the propensity for these patients to die of sudden cardiac death (a lethal heart rhythm requiring a shock of electricity or luck to reverse) rather than acute myocardial infarction (heart attacks). In this study (PDF), from Italy, the investigators found that nearly half of the cardiovascular deaths were due to sudden cardiac death (SCD). The authors retrospectively looked at their data to find risk factors for SCD.
They prospectively looked at 476 patients in 5 Italian hemodialysis units. The cohort was tracked for 3 years and had 167 deaths (35%), 32 due to SCD and 35 due to other CVD. On multivariate analysis they found the following risk factors for SCD: As important as what was significant, is what was not significant. Left ventricular hypertrophy, heart failure and valvular heart disease, all important risk factors for SCD among non-dialysis patients were not associated with SCD in their cohort.
As important as what was significant, is what was not significant. Left ventricular hypertrophy, heart failure and valvular heart disease, all important risk factors for SCD among non-dialysis patients were not associated with SCD in their cohort.
The most interesting analysis was when they parsed out the day of the week the patients died of SCD. Instead of looking at the absolute day they related the day to the patients dialysis schedule. I have modifed their chart to reflect this, with twin X-axis: one for MWF and another for TTS patients. The red line indicates how high the bars would be if there was no relationship to the dialysis schedule. The highest risk periods were the 24 hours before dialysis at the beginning of the week and the 24 hours after the dialysis at the beginning of the week. Not dialyzing for the two days over the week-end put patients at risk for SCD both before and after subsequent dialysis.
The red line indicates how high the bars would be if there was no relationship to the dialysis schedule. The highest risk periods were the 24 hours before dialysis at the beginning of the week and the 24 hours after the dialysis at the beginning of the week. Not dialyzing for the two days over the week-end put patients at risk for SCD both before and after subsequent dialysis.
This sounds like an electrolyte associated complication rather than a uremic toxin because of the risk after dialysis, indicating the change in the toxin, not just the high level, is a risk-factor. This is supported by studies (1, 2) of potassium modeling in which the potassium in the dialysate is lowered sequentially during dialysis. By modeling the potassium, the speed of potassium removal is decreased. This has been shown to decrease pre-mature ventricular contractions (a benign momentary disturbance in the heart rhythm that is being used as a proxy for more serious arhythmias, like SCD. Medicine has gotten in trouble with this proxy in the past so it may not be appropriate.).
Summary: modestly high potassiums are associated increased SCD and the two day dialysis holiday on traditional three day a week dialysis is likewise associated with SCD. Hello daily dialysis!
The lecture on Potassium that this entry was drawn from:
Whats New In Potassium
View more presentations from Joel Topf.
What’s new with hyperkalemia: EKG changes
Today I did a lecture for the fellows on hyperkalemia. It is interesting that nearly none of the content I use to teach the residents and students is used in a lecture for the fellows. Same subject complete rewrite.
I plan on doing four posts on hyperkalemia from this lecture:
- EKG changes
- Dialysis patients and hyperkalema
- Digoxen toxicity and hyperkalemia
- Renal adaptation to ACEi and aldo antagonists in CKD
The lecture started off with the case I blogged about last week with the scary EKG and the potassium of 9.9.

I focused on a well done study (Full Text) by Drs Montague, Ouellette and Buller from Yale. They looked at 90 patients with a potassium grreater than 6 and an EKG done within an hour of the potassium. They excluded hemolyzed specimens and patients with cardiac pacing or other conditions which would mask EKG changes.
They graded all the EKGs according to a prospective criteria and recorded the cardiologists assessment. The average patient was 73 years old (20-93) and half had acute kidney injury (55%) and half had chronic kidney disease (47%). They did not comment on the degree of overlap between those groups. Half the patients had diabetes (55%). Only 31% were on ACEi and 30% on loop diuretics.
The average patient was 73 years old (20-93) and half had acute kidney injury (55%) and half had chronic kidney disease (47%). They did not comment on the degree of overlap between those groups. Half the patients had diabetes (55%). Only 31% were on ACEi and 30% on loop diuretics.
The reading cardiologist documented peaked T waves in only 3 of 90 patients with hyperkalemia. The investigators were able to find peaked T waves in only 29. QRS widening was found in only 6 patients. Of the 52 patients who could have been classified as having “Strict Criteria” (you needed a second EKG after resolution of the hyperkalemia and not everyone in the cohort had a second EKG) only 16 actually met strict criteria. The authors found EKG criteria to be insensitive predictors of hyperkalemia:
The authors found EKG criteria to be insensitive predictors of hyperkalemia:
- Sensitivity of strict criteria: 18%
- Sensitivity of any EKG change 52%
Interestingly, they found that acidosis decreased the likelihood of finding peaked T-waves.
When they looked at arrhythmias as an outcome, EKG changes continued to be a poor clinical guide. They were not sensitive: only one of the patients who subsequently developed an arrhythmia or cardiac arrest had previously met the strict criteria for EKG changes and only 7 had any T-wave findings at all. This is important because it emphasizes the fact that you can not be reassured by a normal EKG in a patient with hyperkalemia.
The study was unable to look at specificity because all of the patients had hyperkalemia. An earlier study by Wrenn, Slovis and Slovis was able to look at sensitivity and specificity because they did have patients without hyperkalemia in their cohort. They retrospectively reviewed the EKGs of 220 patients with either renal failure (n=133) or hyperkalemia (n=87):
- Sensitivity: 39%
- Specificity: 85%
When they restricted the cohort to patients with a potassium over 6.5 the sensitivity rose to 58%.
Take home message: a normal EKG should not rule out hyperkalemia and should not decerase your concearn for impending arrhythmia.
Here is the lecture this post is based on:
Whats New In Potassium
View more presentations from Joel Topf.
Statins fail again
Statins have a tortured relationship with nephrology. Our patients have accelerated atherosclerosis and they die overwhelmingly of cardiovascular disease. So one of my primary jobs is to continually optimize cardiovascular risk factors to save my patients
Control blood pressure, start an aspirin, and maximize the statin are the lather, rinse, repeat of my world.
That said we have little data that this makes a whit of difference, at least in our dialysis patients.
Aspirin
- No randomized trials have been done on the role of aspirin to prevent cardiovascular events among dialysis patients.
- Aspirin was found to increase acute coronary syndrome in an unbadjusted analysis but was not significant in multivariate analysis.
- Berger et al. (PDF), however found a dramatic reduction in 30-day mortality for patients with acute myocardial infarction given aspirin. Unfortunatly fewer dialysis patients received ASA and other standards of heart-attack care (beta-blocker and ACEi) than patients not on dialysis.
 The survival of patients based on whether they received ASA for their acute MI
The survival of patients based on whether they received ASA for their acute MI The use of standard therapies for acute myocardial infarction was lower among dialysis patients, even patients deemed ideal candidates for the therapy.
The use of standard therapies for acute myocardial infarction was lower among dialysis patients, even patients deemed ideal candidates for the therapy.- Aspirin with clopidogrel was associated with a lot of bleeding (number needed to harm was only 5.6) in a trial to prevent access clotting

Blood pressure
- Hypertension, along with cholesterol and obesity, is subject to reverse epidemiology in dialysis patients. This means that observed epidemiology trends are the opposite of what you would expect from data on non-dialysis patients. Lower blood pressure leads to high mortality, lower cholesterol leads to higher mortality, increased BMI yields better observed survival. The observational data, however, does not mean that interventions to lower blood pressure will lead to the same bad outcomes.
- A recent meta-analysis (PDF) of 8 randomized trials of anti-hypertensive therapy gives credence to the practice of treating hypertension in dialysis patients.

- One thing high lighted by the trial, though, is the paucity of evidence for this treatment: They were able to find only 1,679 patients. Terrible.
Statins
- The 4D study is one of the few randomized controlled trials in dialysis patients and unfortunately did not show any improvement in mortality with atorvastatin. The study randomized 1,255 hemodialysis patients to either 20 mg of atorvastatin or placebo. After 4 years they found the statin was safe and effective in reducing the median serum LDL cholesterol level by 42%. However, the primary endpoint—cardiac death, nonfatal MI, and stroke—was reduced by insignificant 8% (P=0.37).

- The authors found a significant increase in fatal strokes among the patients randomized to atorvastatin. (RR 2.03, P=0.04).
- Today came word that another randomized controlled trial on statins among hemodialysis patients, AURORA, was also a bust. Published yesterday in The Journal, AURORA randomized 2,776 dialysis patients to 10 mg of rosuvastatin (Crestor) or matching placebo. The end-point was a composite of CV death, non-fatal MI, and non-fatal stroke. Average follow-up was 3.8 years and there was no difference in the primary outcome (396 outcomes with rosuvastatin versus 408 on placebo, P=0.51).

- AURORA found no increased risk of strokes as found in the 4D study.
Great article on the two new PSA studies in the NEJM
 The New York Times has good coverage of the latest data (US Study, European study) on prostate cancer.
The New York Times has good coverage of the latest data (US Study, European study) on prostate cancer.
I loved this beat which covers the difference between relative and absolute risk and NNT:
[After discussing the 20% reduction in mortality found in the European study] But in terms of individual risk, even that is not a huge benefit. It means that a man who isn’t screened has about a 3 percent average risk of dying from prostate cancer. If that man undergoes annual P.S.A. screenings, his risk drops to about 2.4 percent.
And there is an important tradeoff. P.S.A. testing increases a man’s risk of being treated for a cancer that would never have harmed him in the first place. The European study found that for every man who was helped by P.S.A. screening, at least 48 received unnecessary treatment that increased risk for impotency and incontinence. Dr. Otis Brawley, chief medical officer of the American Cancer Society, summed up the European data this way: “The test is about 50 times more likely to ruin your life than it is to save your life.”
How not to randomize a study
 If you are designing a randomized study, make sure you actualize randomize your patients. Schiffl messed this up in his study of daily versus three days a week dialysis, for acute renal failure. Schiffl achieved randomization by alternating eligible patients to three days a week versus daily dialysis. One key aspect about randomization, especially in non-blinded studies, is that the investigators cannot know what arm of the study the patient will be in prior to enrolling the patient. With alternating patients every investigator knows which arm the next patient will end-up in and they can make subtle decisions on the appropriateness of the patient or in how they present the consent form to influence the composition of the study arms.
If you are designing a randomized study, make sure you actualize randomize your patients. Schiffl messed this up in his study of daily versus three days a week dialysis, for acute renal failure. Schiffl achieved randomization by alternating eligible patients to three days a week versus daily dialysis. One key aspect about randomization, especially in non-blinded studies, is that the investigators cannot know what arm of the study the patient will be in prior to enrolling the patient. With alternating patients every investigator knows which arm the next patient will end-up in and they can make subtle decisions on the appropriateness of the patient or in how they present the consent form to influence the composition of the study arms.
This comes up, because my fellow sent me a paper on prophylactic dialysis prior to CABG (PDF). From the paper comes this gem:
 Repeat after me, “If you know what arm the patient will be in prior to enrolling the patient, you are not running a randomized trial.”
Repeat after me, “If you know what arm the patient will be in prior to enrolling the patient, you are not running a randomized trial.”