


Will the UK courts squash scientific discourse?
 This article about Simon Singh‘s battle with the British Chiropractic Association is frightening.
This article about Simon Singh‘s battle with the British Chiropractic Association is frightening.
The consequences of letting the libel law loose on scientific debate are horrendous. Science proceeds by peer review. A researcher’s colleagues must submit his or her ideas to scrutiny without fear of the consequences. If they think they could lose their homes and savings in the libel courts, however, they will back off.
For alternative therapists are not the only ones answering their critics with lawyers. NMT, an American health giant, is suing a British doctor for questioning one of its treatments.
Incredibly the BCA has won the first legal round.
The BCA sued for libel. And on May 7th Sir David Eady, a high-court judge, ruled, in a preliminary hearing, that the “natural and ordinary meaning” of the phrase (the relevant legal test) was that the BCA was being consciously dishonest and knowingly promoting quack treatments.
 The key to the court case is a claim that chiropractic treatments for problems outside of backpain are bogus that Singh made in Trick or Treatment: The Undeniable Facts about Alternative Medicine
The key to the court case is a claim that chiropractic treatments for problems outside of backpain are bogus that Singh made in Trick or Treatment: The Undeniable Facts about Alternative Medicine, a book he coauthored on alternative medicine.
Advancing medicine and science is impossible if writers have to self-censor themselves when discussing scientific claims.
Nike+ iPod imprecision
 I have been running off-and-on for the last 3 years (mostly off) and running regularly for the past 15 months. I love how lightweight it is the antithesis of biking or backcountry hiking with their emphasis on gear. Running is nearly completely free of equipment and gear. All I do is strap on my shoes, plug in the headphones and go. The exception to this is my Nike+ iPod pedometer. This is a cool gadget that consists of a sensor which goes in your shoe and a receiver which plugs into the 30-pin connector on the bottom of the iPod Nano. If you use an iPod Touch you don’t even need the receiver.
I have been running off-and-on for the last 3 years (mostly off) and running regularly for the past 15 months. I love how lightweight it is the antithesis of biking or backcountry hiking with their emphasis on gear. Running is nearly completely free of equipment and gear. All I do is strap on my shoes, plug in the headphones and go. The exception to this is my Nike+ iPod pedometer. This is a cool gadget that consists of a sensor which goes in your shoe and a receiver which plugs into the 30-pin connector on the bottom of the iPod Nano. If you use an iPod Touch you don’t even need the receiver.
I was blown away by the accuracy of the device and have been rediculously satisfied with this $30 gadget. Two events brought home how accurate the pedometer was: I ran a Cinco de Mayo 5k in Brooklyn with my sister a few years ago. The pedometer signaled 5k on the very footfall that crossed the line finishline. It was accurate to the step. Amazing:
I had a similar experience in the Detroit Marathon Relay in 2007. I ran a short segment from Downtown to Belle Isle. As soon as I crossed the timing blocks the iPod signaled I had reached my goal:
Last fall when I did the half marathon the accuracy fell a bit. It recorded 13.6 for a 13.1 mile route but I felt that 5% slosh was okay:
I had the same over estimate occur during the martian Marathon 10k. With the devic recording 6.5 miles for a 6.2 mile run. Again a 5% error:
 What inspired this post was the new finding that in 2009 the error has swung in the opposite direction, now the Nike+ is underestimating my distance and speed. I first noted this during an 8.5 mile loop I ran with PBFluids reader and fellow nephrologist Steve Rankin. The Nike+ only recorded 7.98 miles:
What inspired this post was the new finding that in 2009 the error has swung in the opposite direction, now the Nike+ is underestimating my distance and speed. I first noted this during an 8.5 mile loop I ran with PBFluids reader and fellow nephrologist Steve Rankin. The Nike+ only recorded 7.98 miles:
Yesterday I did the Dexter-Ann Arbor half marathon and again the Nike+ iPod underestimated the distance and speed:
In the end it was only off by 0.6 miles over 13.1, so 5% but on my next run my Nike+ odometer will cross 1000 miles and its a little less satisfying thinking that I already crossed that milestone at some unrecognized time in the last month or so.
Update: Just discovered that the New York Times recently did a review of the Nike+iPod system.
The Sugar Fix: Chapter One: The Fructose Factor
 Johnson starts The Sugar Fix
Johnson starts The Sugar Fix with the assertion that a century ago heart disease, diabetes and obesity were rare conditions.
In 1890 a survey of 5,000 US citizens revealed that only 3.4% of Americans were obese and they were typically isolated to the upper class. This compares to a contemporary rate of 32%. Two thirds of Americans are either overweight or obese. This includes one third of school children. This obesity rate has doubled since 1976 (CDC Source). The rapid increase in girth cannot be explained by genetics. Johnson feels that the rapid change in the frequency of obesity exonerates genetics as the cause, he states that the human genome has been relatively stable going back a few thousand years.
This leaves an environmental change. He then considers and discards changes in physical activity as the etiology. This is supported by the most recent analysis revealed at the 2009 European Congress on Obesity.
Johnson goes on to implicate fructuse. He states that fructose intake has increased 30% since the 1970’s. Fructose is the main source of sugar in fruit. It is half of the molecule sucrose, table sugar. In 1970 the average American consumed half a pound of High Fructose Corn Syrup. By 2000 that had increased to 42 pounds a year. Though HFCS consumption has risen by two orders of magnitude, fructose exposure has only gone up by 30%. This likely means that HFCS has largely replaced the prior source of fructose in the diet, table sugar. The authors don’t address that inconsistancy in this chapter.
Fructose causes obesity through multiple mechanisms:
- fructose causes more and faster weight gain than seen with other sugars
- fructose does not satisfy your appetite resulting in more calorie intake
- increased fructose dulls the brains responce to the normal satiety signals so that following chronic fructose exposure subjects eat more as they don’t sence “fullness”
- fructose upregulates enzymes which promote obesity
Johnson believes that other conditions have increased in prevalence in lockstep with the increased exposure to fructose including:
- hypertension: 73 million Americans
- diabetes: 20 million Americans (CDC Source)
- kidney disease: 20 million Americans
- liver disease: emergence of NASH, now effect 2-5% of Americans (NIDDK Source)
- metabolic syndrome 55 million Americans
The mechanism linking fructose and these problems comes from multiple metabolic consequences of fructose:
- fructose is the only sugar which increases the production of uric acid which leads to hypertension
- fructose increases the production of triglyceridesand lowers HDL
- fructose causes insulin resistance
- fructose causes kidney disease
This last section is not supported by any references or data but Johnson promises to reveal the details later in the book.
Great spoof ad on the impending Palm Pre
The heavy guy in blue is Roger McNamee, co-founder of Elevation Partners, a private equity group with a huge position in Palm. The video is a riff on episode a few months ago where McNamee caused quite a stir by overstoking the hype on the Pre, from Fortune:
In early March, McNamee caused a stir by telling a wire-service reporter that he thought the Pre was so good that customers would give up their iPhones as soon as their AT&T contracts expired. Palm was forced to file a statement with the SEC calling his comments “premature” and “an exaggerated prediction of consumer behavior.”
The slender guy is Jon Rubenstein, one of the creators of the iPod from Apple and the lead designer of the Palm Pre.
The Sugar Fix: The Introduction
In the introduction of The Sugar Fix, Johnson uses a broad brush to establish the scope and purpose of what he intends to prove in the subsequent 300 pages.
- He gives a brief anecdote about the increasing prevalence of obesity. His uric acid hypothesis is going to explain this huge health problem.
- He outlines how he was initially looking for the cause of hypertension when he realized the weight-loss potential of a low fructose diet.
- He then speeds through a handful of clinical studies, both epidemiologic and interventional, which implicate uric acid as a powerful risk factor for cardiovascular disease, i.e. uric acid as the new cholesterol. He admits that the scientific establishment has not accepted his theory as facts and that uric acid today is where smoking was in the 50s and cholesterol was in the 60s.
He concludes the chapter by disclosing two potential sources of bias. He is the Dr. Cade Professor of  Medicine at the University of Florida and that his salary and research is supported by sales of Gatorade by the PepsiCo corporation. This is an interesting disclosure because the cola companies are the principle villains in this morality tale. I wonder if part of the reason for the release of Pepsi Throwback (sucrose rather than high-fructose corn syrup (HFCS) as the principle sweetener) is the pushback against HFCS partially lead by Dr. Johnson.
Medicine at the University of Florida and that his salary and research is supported by sales of Gatorade by the PepsiCo corporation. This is an interesting disclosure because the cola companies are the principle villains in this morality tale. I wonder if part of the reason for the release of Pepsi Throwback (sucrose rather than high-fructose corn syrup (HFCS) as the principle sweetener) is the pushback against HFCS partially lead by Dr. Johnson.
He also explains that he has applied for multiple patents that could financially benefit him if the relationship of uric acid and cardiovascular disease bears fruit.
(pdf)
Journal Club: Aggrenox and AVG for TZDs in HD
Dixon et al. Effect of dipyridamole plus aspirin on hemodialysis graft patency. N Engl J Med (2009) vol. 360 (21) pp. 2191-201 (PDF)
Randomized placebo controlled double blind trial of patients on hemodialysis or to start hemodialysis in the next 6 months with a new AVG.
Primary outcome was loss of primary unassisted graft patency. thrombosis, 50% stenosis. Patients underwent regular site monitoring and referred for angiography if qB was less than 600 or less than 1000 and a greater than 25% reduction of qB.
Power analysis required 1054 patients.
results: 321 randomized to Aggrenox
328 assigned to placebo
 No difference in bleeding or cardiovascular events.
No difference in bleeding or cardiovascular events.
Take home message: modest benefit from expensive drug in underpowered but well designed and executed study.
Brunelli et al. Thiazolidinedione use is associated with better survival in hemodialysis patients with non-insulin dependent diabetes. Kidney Int (2009) vol. 75 (9) pp. 961-8 (pdf)
Thiazolidinediones (TZDs)
- bind peroxisome proliferator-activated receptor gamma
- increase insulin sensitivity in peripheral tissues
- increase HDL
- decrease triglycerides
- decrease visceral fat
- improve endothelial function
This study is a retrospective analysis of hemodialysis patients in the ArMORR cohort.
ArMORR is a cohort of incident dialysis patients at FMC units. The total cohort includes 10,044 patients.
This analysis restricted to patients with diabetes surviving at least 30 days on dialysis.
Patients on pioglitazone (Actos) or rosiglitazone (Avandia) were placed in the TZD group. Primary outcome was time to death from any cause. Maximum follow-up was one year.
Results: 5,290 patientss were eligible for inclusion.
9.6% were treated with a TZD


Improved survival was seen among patients on TZDs, especially patients not also on insulin. Interestingly the survival benefit came from a reduction of non-CV end-points.
Cool site on eGFR and proteinuria
2009 Annual Evidence Update on Proteinuria and eGFR
This Annual Evidence Update has been created to update the evidence presented last year for the 2008 National Knowledge Week on Proteinuria and eGFR. You can read commentaries on the latest systematic reviews, randomised controlled trials and the 2008 NICE guideline on Chronic Kidney Disease, as well as see what evidence has been produced in the last 12 months for the different topics presented last year. Drs David Goldsmith and Edward Sharples have also picked out the Treatment Uncertainties from the evidence, which have been added to the UK DUETs database.

UpToDate evidence based medicine or not? Not.
A few months ago medical blogger Laika wrote an insightful blog entry summarizing a meme which had been bouncing around twitter regarding whether UpToDate was evidence based medicine or some other entity.
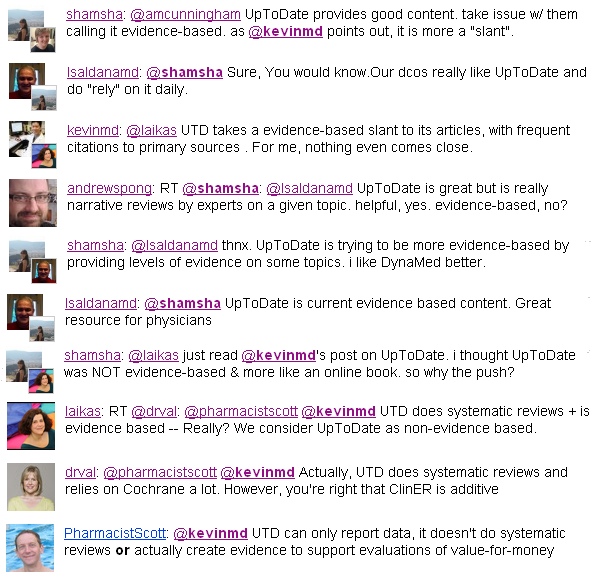
I found the whole excercise to be a bit too philosophical for me. Regardless of what you call it I think everyone would agree that UpToDate is useful. It is a great starting place but usually insufficient as a single source.
I was reminded about it today when I came across this paragraph:
 In the card on “Clinical manifestations, diagnosis, and natural history of primary biliary cirrhosis.” (Link for subsribers)
In the card on “Clinical manifestations, diagnosis, and natural history of primary biliary cirrhosis.” (Link for subsribers)
Regardless of the merits of UpToDate, nothing breaks the illussion of evidence based medicine like an author throwing out a random statistic like “approximately 15% of the 1,200 patients who I have seen…” without a reference. This is the epitome of expert oriented experiential medicine and has no place in EBM.
I am doing Grand-Rounds on the relationship of uric acid and hypertension
 About three years ago I had the privledge to attend a day long seminar on gout put together by Jerry Yee from Henry Ford Hospital. The highlight of the day was a lecture by Richard Johnson from the University of Florida. I had learned about Johnson at my fellowship as the principle discoverer of the link between hepatitis C and membranoproliferative glomerulonephritis (review), in my mind, among the most significant discoveries in nephrology in the last twenty years. Before seeing him I had not made the connection between Richard Johnson and the author of the deservedly popular nephrology text Comprehensive Clinical Nephrology
About three years ago I had the privledge to attend a day long seminar on gout put together by Jerry Yee from Henry Ford Hospital. The highlight of the day was a lecture by Richard Johnson from the University of Florida. I had learned about Johnson at my fellowship as the principle discoverer of the link between hepatitis C and membranoproliferative glomerulonephritis (review), in my mind, among the most significant discoveries in nephrology in the last twenty years. Before seeing him I had not made the connection between Richard Johnson and the author of the deservedly popular nephrology text Comprehensive Clinical Nephrology,
 but it is one and the same.
but it is one and the same.
At that seminar Dr. Johnson gave the greatest lecture I have ever heard. The lecture was on uric acid and its etiologic role in hypertension, obesity and diabetes.
When I heard that he was writing a book on the subject I purchased it and have been reading it on and off for the last 8 months or so. Unfortunately, the book doesn’t have nearly the punch as his 90 minute lecture. My sense is that he writes to the level of the typical purchaser of diet books and comes across more as a carnival barker than one of the most respected researchers in nephrology today.
As I get ready for my grand rounds I am going to blog about uric acid, fructose and the epidemics of diabetes, obesity and hypertension as presented by Dr. Johnson in his book: The Sugar Fix. Should be an interesting ride as the subject is blessed with lots of data, industry influence, huge health implications and a likely Nobel prize if Johnson has really discovered the cause of the bulk of essential hypertension.
