


Apple customer service
I will probably be an Apple customer for life. This past week-end I brought my 16 month old iPhone 3gs to the Genius Bar. The screen has a scratch and a couple of big gouges in it. However, my problem was not cosmetic, the front button was intermittantly not working. In classic repair shop syndrome the button, miraculously healed itself on the morning of my appointment. I brought it in anyways and the Genius changed out the glass in about 10 minutes and the button started working perfectly. Total charge: Zero. Zilch. Nada.
I have had the following genius bar experiences with Apple:
- April 2011: Apple replaces the screen on my iPhone 3gs.
- March 2011: Apple gives me a replacement iPad after I drop and shatter the screen on my year old iPad.
- August 2010 They replaced my Dad’s iPhone 3gs after he got caught in a rain storm and fried the speaker.
- August 2009 My wife’s iPhone 3g broke after a system upgrade. Apple replaced the phone, despite being 13 months old and out of warranty.
- September 2008 My iPhone 3g’s front button became wonky after a trip to the beach. Apple replaced the phone.
- July 2007 My PPC iMac is giving me fits. I bring it in for repair and it is still wonky after getting it “fixed.” I bring the thing back and they replace it with a brand new Intel iMac.
| “Newton… A Mind Forever Voyaging Through Strange Seas of Thought … Alone.” William Wordsworth |
iPhone: the ultimate tool for patient empowerment.
 I walk into a patient’s encounter today and he is reading Twitter on his iPhone 4. We exchanged Twitter handles and began discussing his diabetic nephropathy.
I walk into a patient’s encounter today and he is reading Twitter on his iPhone 4. We exchanged Twitter handles and began discussing his diabetic nephropathy.
I ask how his blood sugars have been and he fires up Glucose Buddy and proceeds to show me all of his blood sugar reading since March of 2010. Then he e-mails me the data.

When we discuss blood pressure, he fires up the iPhone again and shows me iBP. When he sends me his home blood pressure readings I get the choice of receiving them as text, html or CSV. Awesome.
 |
| Glucose Buddy for the iPhone |
 |
| iBP for the iPhone |
Here’s is what the e-mail output looks like:


This was the first patient I have met who is using his phone to document his health. I hope this is a trend because I am sick of patients telling me that they wrote down all of their blood pressures but left the notebook at home. It’s nice to see a cell phone do something other than interrupt a clinical encounter.
Must read article on evidence based medicine
 |
| This is worst Photoshopped pill bottle I have ever seen. |
You don’t see evidence based medicine called out by name often in the lay-press, but Sunday’s Boston Globe dove into the problems with guidelines and quality of evidence in an in-depth analysis. This is a must read.
But evidence-based medicine is only as strong as the evidence used to support it. The stark reality is that evidence can be weak, biased, or even fraudulent. More guidelines stem from expert opinion than from solid clinical trial evidence. And many physicians who write these recommendations have financial ties to drug companies — with no widely accepted policy to correct for conflicts of interest.
More coverage at Cardiobrief.
Cardiorenal Syndrome. Revised
I gave the cardiology fellows at St John Hospital and Medical Center a lecture on cardiorenal syndrome this morning. I revised and expanded the lecture I used for the residents:
- I added my rant regarding the Ronco’s codification of cardiorenal syndrome
- I added the latest NEJM article on diuretic strategies
- I included a section on extracorporeal ultrafiltration and the UNLOAD trial.

It could still use a slide or two on the various loop diuretics and their uses.
We also had an interesting discussion on the data suggesting that loop diuretics maybe harmful in acute decompensated heart failure. I should include a couple of slides on that.
Overall a significant upgrade. You can find the lecture in the usual place.
Best lecture ever
On the subject of lectures, if you haven’t seen Robert Lustig‘s lecture on Sugar: the Bitter Truth, stop what you are doing and find 90 minutes to watch it. Fantastic lecture. Amazing how good his lecture is with such pathetic slides. It’s not about the deck.
The New York Times is running an excellent profile of the lecture (Really? Sunday New York Times Magazine profile piece on a lecture?) this Sunday. Gary Taubes wrote the profile, he is the same author who wrote the best article I ever read on the science and politics of the Atkins diet back in 2002.
Take the time to check out the lecture and the profile.
IVF and Sodium handout updated
I rewrote large sections if the IVF and Sodium handout. I added Tea and Toast syndrome, more on SIADH and a lot of interactivity. Overall a huge improvement. I used it today with the Beaumont Hospital Family Practice residents and was really pleased. Find the update in the handouts tab.
Patient list
Yesterday:
- My first patient had SIADH and a sodium of 125
- My last patient had nephrogenic diabetes insipidus and a sodium of 150
The statistician in me, looked at the patient list and concluded, normal sodium.

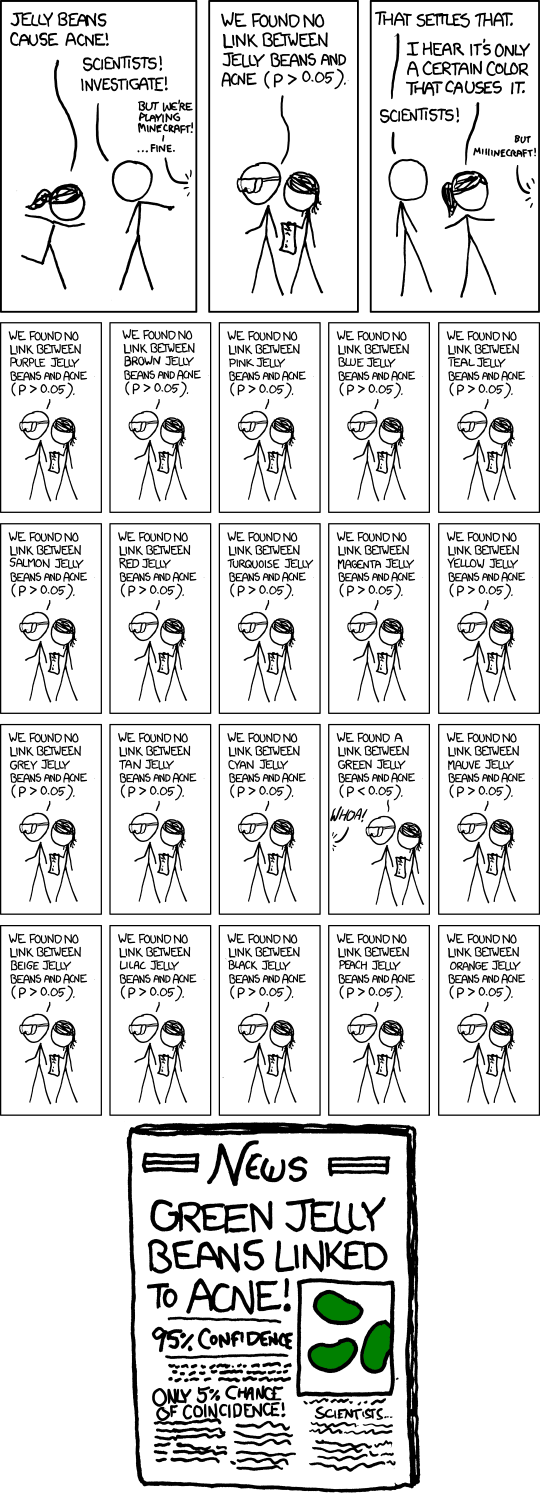
P less than 0.05
Lecture on how to give a lecture
This post really resonates with me: The Ten Commandments of PowerPoint and I wish that I had included it in my lectuer from last week on how to give a lecture.
The chief resident at St John Hospital and Medical Center asked me to do morning report on giving better presentations. It was an interesting project. I have been pretty busy and didn’t have enough time to put together a really polished presentation, but this is what I came up with.
Here is a link to the PDF and Keynote file (130 mb)
iWork documents are a little wonky if you are not using Safari. So the videos I embedded in the lecture are below if you are having trouble looking at them.
Steve Jobs tells it how it is regarding Microsoft
The birth of a morning report:
Screen captures with command-shift-4:
Smart builds
Highlight text:
Mask an image
Improve a crappy figure: