I gave a lecture on HIV renal disease to the ID section yesterday. I give this lecture every couple of years. I swear that lecture changes more from year to year than any subject I talk about.
The lecture was about one hour.
The section on APOL1 is rough.
I would like a slide describing the transgenic mouse model studies by Klotman that showed that transcription of nef and pol are central to the disease.
I need some notes on why I have 2 graphs on slide 16.
Add some highlights to table in slide 23.
Loved how slide 26 and 27 worked.
I think there might be better data on steroids in HIV. Slide 51.
Need to flush out IRIS and DILS from slide 67
Add comment on adefovir slide mentioning that the hep B dose is a sixth of the anti-HIV dose
So last week I asked how you would dialyze the patient in the following scenario:
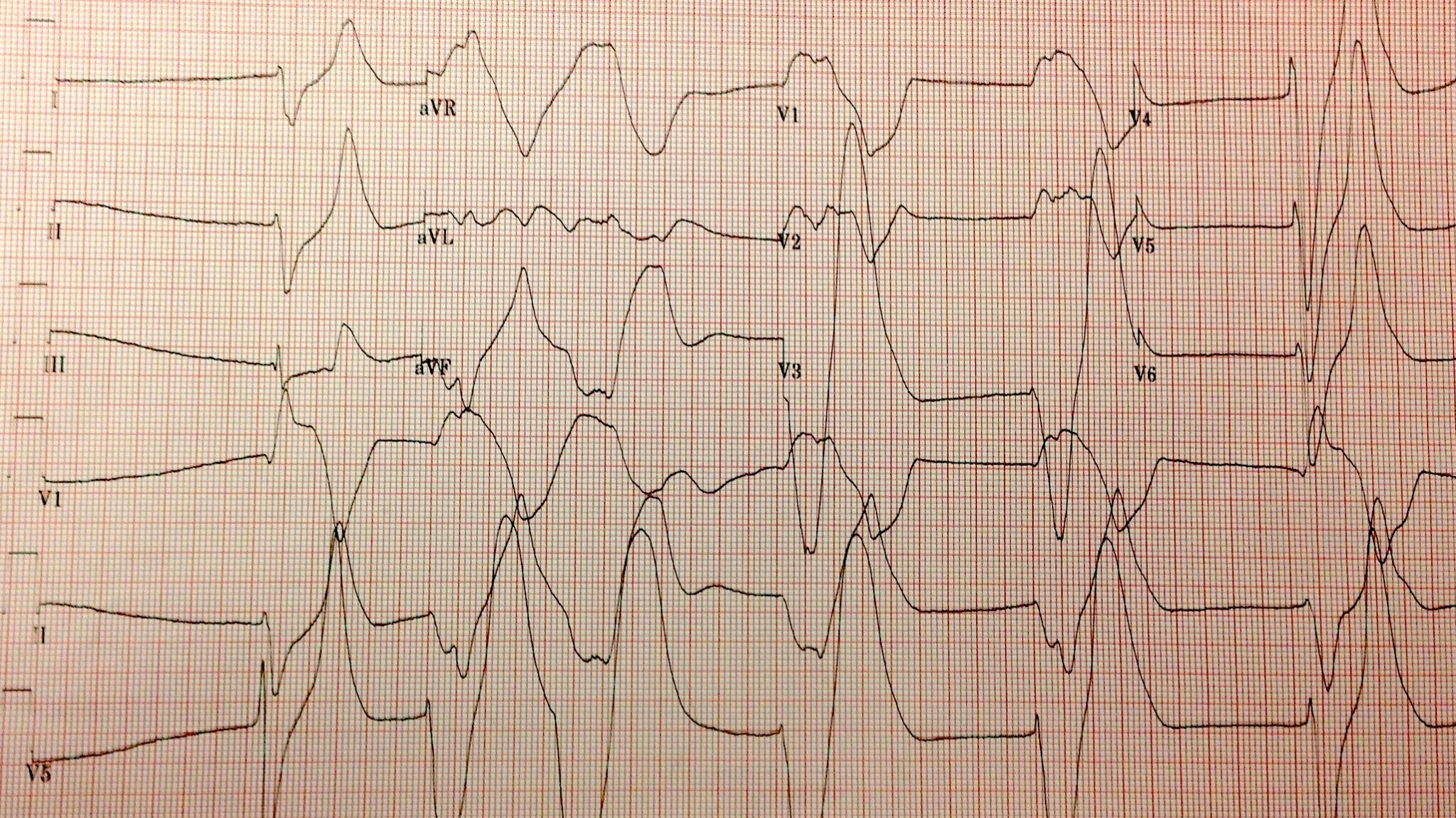
You have been called on a Sunday night for emergent dialysis in a patient with hyperkalemia. The patient is a MWF dialysis patient and had a normal dialysis session on Friday. Her ECG on admission is absolutely terrifying and her potassium is 9.9 (hemolyzed). The blood sugar on admission was 965. When you arrive, with K-machine in tow, the patient has been on an insulin drip for an hour and the potassium is down to 5.2
I have received 54 responces and the results have been pretty stable from the beginning. By far the favorite option was to pack up the dialysis machine and head back home. No dialysis for you.
I don’t see any signifigant trends based on background of the provider:
The raw data is available for perusal here. And you can keep voting here.
That is not how I voted. I voted for 2 hours on a 2K bath. My feeling was that the ECG showed dramatic cardiac toxicity and though the emergency seemed to be over, with a repeat potassium of 5.2, I had no guarantee the insulin drip would continue through the night. If it was stopped, intracellular potassium could diffuse back out of the cells. But what really pushed me was the fact that he is scheduled to receive dialysis in just a handful of hours anyways. If I just push that schedule up and dialyze him tonight I provide an extra margin of safety for his potassium and improve my sleep hygiene. No nightmares of lost IV access for the insulin drip.
Because I viewed this emergency dialysis as just pushing forward the scheduled dialysis I went with the standard 2K dialysis bath.
Now for the best part of any blog post, belittling people who don’t agree with me. The above paragraph takes care of no dialysis.
Zero K bath. Too great a risk of hypokalemia. We presume that he does not have excess total body potassium, merely maldistribution of intracellular potassium. Zero K baths are dangerous. Who can forget the classic scene in Grey Anatomy where Izzie is fired for ordering a zero K bath, putting a patient in shock, so that the poor dialysis patient misses her transplant. (I love that show, they even let surgical residents write dialysis orders.)
One K bath. See above. Though the concern about the toxicity of low potassium baths seems to be overblown.
Two K bath. Perfect.
Three K bath. Should work just fine.
Four K bath. What’s the point, at the current potassium of 5.2, two hours on a 4 K bath will remove a trivial amount of potassium and is functionally identical to no dialysis at all.
The fluids book is certainly priced right (free) but if you need an additional endorsement, Richard Sterns, the Dean of Sodium, uses figures from the book in his talk at the ASN board review class!
One of my colleagues pointed me to your website today. I don’t know that you’re right about me being the “Dean” of anything, but you are correct: I loved your book. Hope you don’t mind that I borrowed from it.
Rick
Richard H. Sterns, MD Chief of Medicine Rochester General Hospital 1425 Portland Avenue
My son is doing a big project on the kidney. As part of that project he has to write a limerick about the kidney. The family was stumped so of course we decided to crowd source the problem:
My son has to write a kidney poem. What rhymes with dialysis? — Joel Topf (@kidney_boy) April 18, 2013
The answer was analysis and paralysis (hat tip to @emmadalton and Leon)
But the real fun began as people sharpened there pen knives and carved new limerick’s on to the bathroom walls of twitter.
@kidney_boyThe news is sad.We’ve done a urinalysis.Your kidneys are bad.You will need dialysis. — Skeptical Scalpel (@Skepticscalpel) April 18, 2013
@skepticscalpel @kidney_boy In retrospect, there must have been a diagnosis we missed…Meh, oh well. Let’s get you on the UNOS list. — Michael Katz (@MGKatz036) April 18, 2013
@mgkatz036 Stop that NaClits the reason he’s not doing wellIn order to volume resuscitateThe hip new thing is Ringers Lactate — Joel Topf (@kidney_boy) April 18, 2013
Kidneys, most of us have two.Some have one, shaped like a horse shoe.Can’t live with none,Dialysis or transplant have to be done. — Vijay(@scanman) April 18, 2013
A man was once stung by a beeHe thought he got off scott freeBut he had rhabdomyolysisAnd now he’s forever on dialysis — Joel Topf (@kidney_boy) April 18, 2013
Daughter noted spelling error (now instead of know)
@kidney_boy if only his doctors weren’t second rate.they couldn’t afford up-to-date. — Michael Katz (@MGKatz036) April 18, 2013
Kidneys are shaped like a beanThey keep your blood cleanThey are the coolest organ unseenUnless you open the body and that would be mean — Joel Topf (@kidney_boy) April 18, 2013
Daughter wrote that one.
When your kidneys failNo need to wailCause in the final analysisYou can always try dialysis — Joel Topf (@kidney_boy) April 18, 2013
My son is pretty independent and ignored all of the bad poetry advice on Twitter and went with this original creation:
There once was a kidney named Bud He liked to filter the blood He got a disease There’s pus when he pees And now Bud is simply a dud
Keep in mind this was a coordinated campaign involving one central blog but generated posts on at least four other blogs, had a single Twitter account but ultimately had 75 people on Twitter using the hashtag.
I really would appreciate any thoughts about this. Please tweet @Kidney_boy or fill in the comments below.
Posted on
I did this interview for eAJKD. I met Jamie Dwyer once, and though he was charming, well spoken and clearly intelligent the overriding biggest impression was that he was best dressed nephrologist I ever met.
…however, it was a hemolyzed specimen so it is a tarnished victory. The patient is a dialysis patient in DKA and had a blood sugar of 925 at the time of the hyperkalemia.
I love that the only things not circled are a creatinine of 8.9 and BUN of 50.
The patient was started on an insulin drip and one hour later his potassium was 5.2 mmol/L. A drop in the serum potassium of 4.7 mmol/L is profound and atypical. This is due to two factors:
The initial serum potassium was not that high, despite the subtle EKG changes the real potassium had to be somewhat lower and falsely elevated due to the hemolysis.
In DKA the hyperkalemia seen on presentation is due to a transcellular shift of potassium from the lack of insulin and increased extracellular osmolality (from the hyperglycemia), both of these are quickly reversible with IV insulin.
Adrogue et al created a formula to predict the potassium at admission in DKA.
K+= 25.4 – (3.02 x pH) + (0.001 x glucose) + (0.028 x Anion Gap)
The calculation is a totally failure in our patient: it comes to a predicted potassium of 5.6. Though the equation is not very predictive (R2= 0.25), the article does a nice job reviewing the mechanisms of hyperkalemia in DKA. This is a concept that is commonly misunderstood. Medical students are quick to rely on the mechanism of potassium moving out of cells in exchange for hydrogen moving into cells in the face of acidemia. Adrogue reviews the data that shows that this does not occur with the organic acids of DKA or lactic acidosis but that acidemia does inhibit the Na-K-ATPase.
Nice picture but this in not an important mechanism in the hyperkalemia of DKA.
The reason that acidemia does not generate hyperkalemia in DKA, is that the anions move into the cells along with the hydrogen ions, so there is no need to excrete potassium to maintain electroneutrality.
Horacio E Adrogue
Funny story about Adrogue, I was eating breakfast at Kidney Week in 2011 when I looked at the name tag of the guy sitting next to me, it was Horacio Adrogue! My chin hit the floor and I started to gush about how much I respected his work and how I loved his NEJMelectrolytereviews and how I was hoping he would autograph my chest and could I pick up his dry cleaning and… then he interrupted me to explain that he was not the Adrogue I was looking for. He was, in fact, The Man’s son and a transplant nephrologist of some regard. How humiliating.
A nice review of the hyperkalemia and hyperglycemia in dialysis patients was published a couple of years ago by Tzamaloukas, a widely published investigator on the subject. I love this figure from the review which shows a curvilinear relationship of glucose and potassium in dialysis patients.
Nice graph except for micromoles of potassium per mmol of glucose. Really? Could you make it more obtuse?
One of the interesting conclusions that I learned from the review: one of the most important variables which affects how much the potassium will fall with insulin is the pre-treatments potassium level, the higher the potassium, the greater the response to insulin. The data from that conclusion comes from this study: Serum potassium and acid-base parameters in severe dialysis-associated hyperglycemia treated with insulin therapy. It is an analysis of 43 episodes of hyperglycemia, half DKA and half non-ketotic hyperglycemia. Here is the money shot showing the relationship to initial potassium to drop in potassium:
What would you do for this patient?
I will share the results in a week or so.
Addendum: some of the funnier tweets in response to my original tweet:
William J Stone is Chief of Nephrology at the Tennessee Valley VA and faculty at Vanderbilt Medical School. He discovered beta-2 microglobulin amyloidosis in long term dialysis patients. He describes the discovery here:
I discovered B2M amyloid in 2 hemodialysis patients during the late 1970’s and early 1980’s who sequentially broke both femoral necks. We were doing home hemodialysis on 75 VA patients, who lived an average of 220 miles away. One of them had a cystic knee lesion, which we biopsied. It was Congo red positive. A light bulb went off in my brain. All of the femoral neck tissue from both patients at joint replacement, misread as increased connective tissue, was full of amyloid. Workup for AA and AL was negative. The patient later died of lung cancer. At autopsy we scooped the amyloid out of a large humeral lesion. When sequenced in NYC, its subunit was intact B2M. To my knowledge, this has not been repeated.
In the early days of dialysis he was in Vietnam with Army and used dialysis for battlefield injuries, Stone again:
I was sent to the Third Field Hospital in Saigon from 1968-69, where we dialyzed battle casualties and falciparum malaria cases of AKI. I had completed a basic science nephrology fellowship at Cornell from 1965-67 and had never done dialysis before. We saved a lot of them using the old coil dialyzers.
One of his former fellows described him as, “One of those guys who can describe a case of almost anything you can imagine, across all of internal medicine.”
Dr. Stone has created the Rules of Stone, bits of wisdom that should guide doctors through the uncertainties of diagnosis and treatment.
Rules of Stone
Anything can do anything. (WJS clarified: is for people who say things like a stroke alone cannot give you a high fever)
Anything can do nothing. (WJS clarified: is for those doubters who say a patient on prednisone will have a tender abdomen if he has perforated an ulcer or a diverticulum)
Nothing can do anything. (WJS clarified: refers to self-inflicted illness; e.g. IV injectors of dissolved pain pills can have multisystem disease)
Nothing works every time.
No lab or diagnostic test is perfect.
No disease is always predictable.
Just because you can do something doesn’t mean you should do something.
A patient known to have x,y, and z doesn’t necessarily have x, y, and z.
A person with an illness similar to a previous one probably has it again.
No list is complete.
The more drugs there are for a disease the less likely they are to benefit it.
There are no uninteresting patients (just disinterested physicians).
Four drugs are more toxic then two.
Always guess 20% if you don’t know the real answer.
No drug has been proven useless until it has been tried in scleroderma and ALS.
Just because you failed to diagnose the cause of X in the past doesn’t mean you shouldn’t try again.
Orneriness is best treated as an outpatient.
If an older doctor writes an axiom or a diagram on a piece of paper, ask if you can have it.
Common but unrelated diseases co-exist at least 1% of the time.
If asked when you last played basketball, be able to answer with a day of the week.
Before addressing non-compliance with diet and medicine #1, doctors add medicine #2.
In a sick patient without a diagnosis, get invasive early.
You cannot learn medicine at home, so the new residency hours rules make no sense. A cadre of doctors with inadequate experience is being created.
Hyperglycemia causes pseudohyponatremia. The sodium is diluted by the osmotic movement of water from the intracellular to the extracellular compartment. I was taught the Katz conversion to correct the sodium, the sodium falls 1.6 mmol/L for every 100 mg/dL the glucose is over 100. This comes from purely theoretical work and was published in a letter the NEJM in 1972.
In the 1999 Hillier et al published empiric data that showed the ratio to be 2.4 rather than 1.6.
When ever I encounter hypernatremia I use both formulas and I consistently found that the Hillier estimated the final sodium. I wanted to do a study where I looked at hyperglycemia in dialysis patients and measured estimated final sodium versus actual final sodium to see which calculation worked better. It is a compelling study cohort because the lack of urine output guards against renal losses, a potential source of error. Well, the study has been done. Tzamaloukas et al, published a nice study of hyperglycemic dialysis patients and found the ratio of change in glucose to change in sodium was 100:1.5, almost exactly the same as Katz’s calculation and consistant with my experience.
The y-axis is the Katz estimate minus the actual final sodium. so a perfect estimate is zero. The x-axis is the average of the Katz and actual final sodium. The Katz conversion work well across a range of actual sodium levels.
Eat it Hillier.
Update, Dr. Rondon, in a comment below and Martijn vd Hoogen on Twitter, believe that I made a mistake calling hyperglycemic hyponatremia, an example of Pseudohyponatremia. There is some precedent for this position but it is not universal. See this editorial by the American Association for Clinical Chemistry, or McGraw Hill Concise Dictionary of Modern Medicine
We care about the serum sodium because of its effect on serum tonicity. When the serum sodium doesn’t represent the serum tonicity, the sodium is lying, I call that pseudohyponatremia. Pseudohyponatremia comes in two varieties: normal osmolality and high osmolality. The high version is what I am talking about in this post, the low version is what Drs. Rondon and Martijn vd Hoogen are referring to in there comments/tweets. More information on that can be found here.
@kidney_boy is this pseudohyponatremia? I thought this is dilutional hyponatremia, like mannitol. Pseudohyponatriemia is lab test error.
— Martijn vd Hoogen (@MWF_vd_Hoogen) April 14, 2013