Hospice and palliative medicine has been on my mind a lot recently. Of course, this is partly because it is a region in NephMadness but also because so much of the day to day work of a nephrologist deals with the end of life.
Have you ever read a journal article and as soon as you finished the abstract you had this forbidding feeling that if the authors actually proved what they claimed to have discovered your medical life will never be the same?
In this study the entire cohort showed a survival advantage with dialysis care but on further subgroup analysis, patients over the age of 80 did not gain additional time on earth by choosing dialysis. In this case dialysis did not extend life.
Nephrologists need to start to train ourselves away from the reflex that dialysis is a way to extend life. In some easily identifiable patient groups it provides as much harm as benefit. And this is just counting days alive. If you compare the quality of those days, perhaps by looking at Tamura’s Functional status study, dialysis begins to look especially grim.
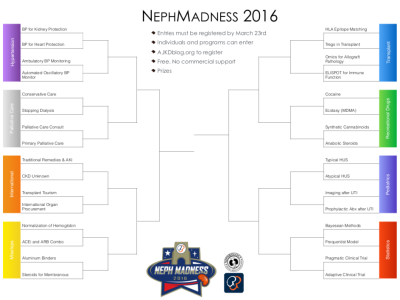
This makes me happy that Palliative care is a region in NephMadness. NephMadness is an online, social media-engaged, medical education project in its fourth year. It is an homage to the NCAA basketball tournament, March Madness. We replace the teams with a bracket full of 32 different nephrology concepts from 8 different academic regions.
Then we replace the games (which normally decide the winners) with a blue ribbon panel that votes on each contest and selects the teams that advance through the brackets.
Participants are invited to fill out their own brackets and see how well they match up against the Blue Ribbon Panel. There are prizes and bragging rights at stake. And no we aren’t nerds. Why do you ask?
Tonight’s chat is going to examine the 4 concepts in the Palliative care region, each for about 15 minutes. The four entries are:
Conservative care
Stopping Dialysis
Palliative Care Consult
Primary Palliative care
Take a look at the brackets, fill out your own and then join us tonight to discuss the Palliative care region.
The AJKDblog runs like a watch. Two posts a week, every week. One on Tuesday, one on Thursday. That steady tic-toc pattern is only broken a few times a year. One time during ASN Kidney Week where they publish as many posts as they can and then again during the NKF Spring Clinical Meeting. Between those events the only other time they break their rhythm is NephMadness. I love how your e-mail inbox is suddenly filled with nearly a dozen fresh posts.
We are grateful that the editors at AJKD trust us to take over the blog for a few weeks to conduct this preposterous idea. We are also thankful that the editorial support team is so committed to this project that they are wiling to reformat the blog to best fit the nature of our content. Thanks AJKD.
In that bounty posts, some of the content can get lost. The regional orientation posts are all quite good, so don’t miss those. Paul’s introduction and explanation of NephMadness is also great and by being published a few days before we unleashed the rest of NephMadness it was well positioned and received a lot of exposure. Matt and I wrote a post that describes the why behind the what and how of Paul’s post. I encourage the curious to check it out. Last year’s why ultimately became the message behind my dotMED and I suspect the idea inside this years post will similarly get expanded at some point to a full blown oral presentation.
Thanks for supporting NephMadness and get those brackets filled out!
In the early days of blogging people would write posts and then other bloggers would comment on the post on their own blog, it was like decentralized comments. So my previous post about the jaded medical student was a post about a blog post, and now Robert Centor, one of the grand wizards of medical blogging has also commented on the same post and mentions my post. Predictably, he has a more productive response than I did. Take a moment to read it.
The written commentary on various blogs brings me back to 2006.
KevinMD has a new post that busts the lid off of medicine. I have reproduced it here with translations from pity party to what the little twerp is really thinking.
It is February of our last few months of clinical rotations. I am a rising fourth-year medical student at a well-known East Coast institution with a not-so-bad track record, I guess you could say. I scored in the top percentile for the USMLE Step 1, honored my third-year rotations, and have comments from attendings about how I am destined to succeed in this career.
Translation: I am smart, good looking and destined for greatness, so the story I am going to tell you if doubly tragic.
One might think that at this point in my life, I should feel confident, well-accomplished, and hopeful for the future. In the last month, there’s been a lot of talk about residency and deciding on a specialty. To me, this meant finally looking back onto my life, my experiences, and all that medicine has meant for me. And I can’t help but feel that I have made a terrible, terrible decision.
Let me tell you all I’ve learned from my long travels and deep experience, from the guy who has almost finished medical school.
I have always dreaded, but predicted, this outcome for me in medicine. I know I can make fickle decisions. I didn’t think medicine was one of them. I was an extremely diligent student for all of my life; I follow and play by rules very well like most others in this field. A lover of biology since grade school, I never saw another path for myself. I heard about medicine’s long journey, and many people (and many doctors) had attempted to dissuade me in all sorts of ways: the infamous “scary” cadaver lab, the years of schooling and residency, nights staying up to study and work, the broken health care system, the inevitably jaded fate of many physicians these days. I was a non-believer. I did not think it would happen to me. And onwards I went — learning what patient care and rounds are like while volunteering as a pre-medical student, studying for months on end for the MCAT, taking years off after Uni to continue my dream of becoming a doctor.
I knew I would be jaded and cynical by the end of medical school but let me tell you how I was diligent and optimistic. And you know I am especially deep because of my strategic use of the passive voice.
Now, I am almost there. I am almost a doctor. I stand at the intersection of many specialties. The difficulties in this choice tell me that I am probably not fit, ultimately, for a career in medicine. I learned that the sacrifices to become a doctor continue into the later years of this career. I learned that there is no such thing as job stability (residency and fellowship are each opportunities to get utterly uprooted from your life). I learned that internists, the quintessential doctor that I grew up admiring, do not have my dream job. I learned that too often do doctors, in general, have to fight the broken system, but internists especially. Broken patients. Broken insurance. A broken health care compensation system that prioritizes crisis intervention, and does not pay doctors to use their intelligence, skills, empathy and sense of humanity to really care for patients.
And can you believe it, the way I dreamed medicine to be is not the truth? Aren’t all careers exactly the way they are portrayed on TV? I guess I should have payed attention to my surroundings during those years volunteering in the hospital. Maybe I was supposed to learn what being a doctor was like rather than just recording those hours away for my application to medical school.
And that brings me to my next point: empathy. I entered medical school so that I can care for others and make connections with complete strangers in the most vulnerable time of their life. I learned that empathy, in general, is not rewarded in medicine. On rounds, I learned that empathy, and a person’s humanity and suffering, is not spoken about (but we will talk on and on about the patient’s rise in creatinine, hyponatremia, etc.).
The only way to measure reward in medicine is in dollars. So that “thanks” and the hug you get from being empathic to a patient or their family means nothing. Only dollars and honors matter. This sucks.
And so, medical students learn quickly how to play this game. We enter noble. We leave jaded. We leave seeing that the smart move is to get out of it. And so the smartest of the smartest, the ones lucky enough to have a choice, go into fields where they limit their involvement with patients: dermatology, radiology, ophthalmology, anesthesiology. It begs the question: why are these the happiest, the most high-salaried, and patient-limited specialties? They all must have a connection.
Remember choice only goes to the lucky ones, not the ones that study, do well, or score in the top percentiles of their boards from a well-known East Coast Institution (who knew that east coast institution was capitalized?) And I am going make happy = rich because it satisfies my thesis that all doctors are money grubbing capitalists and only in it for the cash and ignore data that these non-patient contact specialties are not the most satisfying (Medscape Survey):
The winning card of this game was flashed to me early in my third year. I saw that the internist can stay up all night caring for the ICU patient on the brink of death, and have half the job satisfaction (and half the pay) of the dermatologist who sleeps in on Saturdays and refuses to come in for an urgent derm consult. Compensation shouldn’t be the end-all, but numbers tell you how much society values you. And when this doctor-to-be sees that the values that brought individuals into medicine have seemingly vanished in the residents and attendings that he works with, and is not talked about anymore after the interview to get into medical school, he feels like he’s been completely duped.
“Numbers tell you how much society values you” That is why Donald Trump is highly valued and respected and Malala Yousafzai is a worthless peice of shit. See how smart I am. Top percentile on boards. Top school. Got it all figured out.
Gone like smoke, like we’re all in some sort of circus funhouse. Except it’s not fun. It’s jarring, scary, disappointing, and absolutely depressing. But more than being afraid for myself, I am scared for our future doctors, because I know I am not the only one that feels this way.
Being an adult is hard and scary and there is no way for doctors or anyone to change the reality it was decreed by some higher power to be this way. So instead I’m going to get out and run to Wallstreet as fast as I can and cash in this MD degree. This essay is just one step in my self justification so I can sleep at night.
The author is an anonymous medical student.
Sign my name? Stand up for what I believe? What do you think I’m dumb? Didn’t I mention that I got top board scores from an exclusive east coast university.
35 year old alcoholic. Severe hyponatremia with a sodium of 119. The sodium was corrected over 5 days from 119 to 135. A rate of only 3 mmol/L/day. Patient developed CPM on the sixth day.
Kenar has a nice post on this case with an alternative approach to try to protect patients.
I’m addicted to podcasts. One of my favorite medical podcasts is BS Medicine. The hosts have deep medical knowledge and an enviable commitment to evidence based medicine. In addition, they approach the podcast from a clinicians perspective and don’t get so lost in the science that they forget we are here to help patients.
For their 300th podcast they did a special episode surrounding the dorm room question: If you could have only 20 medications, what would they be?
They had an interesting list and they spoke extensively justifying their list. The explanation and the list stretched over two episodes. Afterwards they did a third podcast to go over the next 10 medications that barely missed the cut.
I loved the thought exercise but I thought James, Mike, Tina and Mike really missed the boat on a few. Here is their list and mine:
The list is the same through the first three, but then I added normal saline. How can you include epinephrine and not include normal saline? And don’t start with me that salt water is not a drug. Saline will cure everything from a hangover to cholera. Essential medication.
They included oral contraceptives. My feeling is that 99% of the function of OCPs could be replaced by IUDs so women could continue to have control over their bodies and I get an additional medication. I will give up treating dysfunctional urterine bleeding, PCO and other maladies that benefit from OCPs.
I also skipped diphenhydramine. If the allergic reaction is bad enough, then we’ll give epineprine, otherwise tough tootles.
I used pentoprazole rather than omeprazole because I wanted an IV formulation. I skipped the losartan and added apixiban instead. I just couldn’t leave all those people with pulmonary embolism, atrial fibrillation and DVTs to fend for themselves with aspirin alone. The losartan omission is a bit tough to stomache as a nephrologist but truly most of the advantage of ARBs can be duplicated with good blood pressure and glycemic control (at least in diabetics). And the other renal diseases tend to be rare. Additionally I’m not as convinced as the podcasters that ARBs are just ACEi without the cough. I can’t remember seeing ARB heart failure data as impressive as:
Consensus Trial Grade 4 CHF, 1988
I don’t know enough ID to vet their antibiotics so I accepted their argument and brought in all three of their antibiotics.
That left me with three more medications after I gave the heave-ho to fluconazole and PEG. To fill this I hadded drugs to treat three of the great infectious diseases that plague this earth: HIV, TB and malaria. Seems morally wrong to ignore them. HAART is one of the greatest medical advances in our lifetime. They have an NNT that approaches one. In 1995, 55,000 Americans died of HIV and they died at young, productive ages causing incalculable losses to the nation. Blood pressure and heart failure medications are hugely important therapeutic target but treatment primarily benefits people in the tail end of their lives. Treating infectious diseases needs to be prioritized because of the age of the people affected.
What’s your list?
— Update —
I received this tweet:
I think he is exactly right. I can use heparin IV or subcutaneous. In this 20 medicine restricted world, thrombophilia will be treated like diabetes, all subcutaneous injection, all the time.
I was on vacation when I got a DM from Ronan Kavanagh asking me if I would be interested in speaking at dotMED. I said yes without really knowing anything about the conference, but a quick glance at the previous speakers convinced me that speaking there would be a once in a lifetime opportunity. A chance to punch above my weight.
Ronan gave me a blank slate to speak on anything I wanted. I chose social media opportunities in medical education.
My wife and I took a red eye to Dublin and arrived on the Tuesday before the conference. We toured the Guiness Factory Store, Kilmainham Gaol, the Modern Art Museum of Ireland and the Irish Museum. On Wednesday night we were invited to the White coat ceremony at UCD. Pat Murray my old program director at University of Chicago is now the dean of the medical school. Friends in high places and all that.
Phenomenal.
The following day I gave a lecture on social media to the staff and students at UCD. Great response.
Big thanks to @kidney_boy who gave an excellent presentn on SoMe & MedEd. You guys attending @DotMedConf are in for a treat.
And it was great getting a chance to rehearse my dotMED talk in front of a live audience.
The talk went long, about 45 minutes for my 30 minute slot. When I went to the Smockalley Theater later that day for an AV check, I asked Kerry O’Sullivan if a slightly longer presentationwas okay. She turned ashen. I had my answer. So I pulled out the metaphorical scalpel and started my lecture lobotomy.
Ronan welcomed everybody and then John Greally, pediatrician and geneticist from Albert Einstein, gave the first talk of the day Learning from Artists in the Digital Age. It was an amazing talk. He started with a history of visual representations of data. From primitive maps, to the first histograms, to maps with epidemiologic data. Fascinating. He reminded us that modern radiology images are just visual representations of what is really quantitive data.
The history lesson was a set-up for the fact that all advances in data visualization occurred before 1900 and that with the era of big data we need new data visualization techniques. He is spearheading this effort by bringing together artists, data illustrators visualizers and geneticists to comb through big epigenetic data dumps to find unique and useful ways to present it to clinicians and scientists. (Nice NYT article about Greally’s efforts).
I loved John’s definition of big data: any data set too large to fit on a laptop.
OMG. Unbelievably good presentation. How did I get placed after John? This could get ugly. #dotmed16
One of the best arguments in favor of social media was made by John. He discussed that forensic statisticians do a lot of the post publication peer review of big data research and they typically publicize their work via social media. I did get the final question of the session and my wife says it was the best part of the morning:
Next up was Leticia Ruiz Rivera discussing her photo exhibit, Limits, which explores the brutality of medical training. She takes portraits of residents before and after their 24-hour shifts. She gave a 5 minute introduction and then we went upstairs for coffee where we could look at her photo exhibit.
After the combination coffee break and photo exhibit the conference resumed downstairs with a Pitch off. Four start-ups in the health space competed to win the conference.
The first company was Humane Engineering with their app Cove. Cove is digital diary that allows you to create music to fit your mood and acts as a non-judgmental, always available, grief counselor. It was an amazing presentation and my personal favorite. As we spend more and more time staring at our phones, reimagining them as tools for psychotherapy seems innovative, important and the type of idea that could change the world. One day psychotherapy will delivered via computer and I don’t know what it will look like but if it is done well and is effective it will be a great thing.
The next company was N-Silico that had an EMR-like product that focused on a specific type of meeting that seemed to me to be like a tumor-board meeting. They developed software that would help the team mates collaborate. It maybe a great idea, but seemed like JAFEMR (just another fracken EMR). Though he did have the best line of the conference, “Paperwork wouldn’t be so bad without the paper…or the work.”
The third presenter was the Beats Medical. They have a smart phone app that treats Parkinson’s disease. Apparently the shuffling gait and freezing can be ameliorated by a metronome like beat. This company has created an app than takes a 2 minutes walk test (done by shuffling around with the phone in your pocket) and then creates a custom metronome beat for your disease. It is customized for the individual in pitch and tempo. This was my wife’s favorite and she was not alone:
We should probably stop the pitches and give @BeatsMedical the prize. Sorry everyone else. #dotMED16
The judges were concerned that this was a defensible idea and that copycats would flood the market. Also it is hard to build a business around the App Store. People just don’t like to spend a lot of money on apps.
Concluding the contestants was PMD respiratory. They build a device that you stick on a patient and it records the respiratory rate. The pitch is that respiratory rate is an important vital sign that can predict bad hospital outcomes but since the rate is poorly measured and recorded we need a way to automate it. Myles Murray gave the pitch and the core to the pitch is that if you look at a ward full of 20 patients, 19 will have a recorded respiratory rate of 16 and the last one will have a respiratory rate of 32, and she’ll be about to code. There has to be a respiratory rate between 16 and 32.
I had never heard of this Panti Bliss, but the story that I pieced together at the conference is that he is a gay, cross dresser and actor. After one of his performances he came on stage and made a impassioned plea for gay marriage. This video went viral and he became an accidental spokesperson for the ultimately successful gay marriage movement in Ireland.
If u click on troll’s profile they have about 4 followers 😂😂😂 @PantiBliss on social media trolls hateful people have few friends #dotmed16
Muris focused the interview on Rory’s HIV status. He turned positive in the mid 90’s and lived through the birth and maturing of the HAART era. Rory discussed the wonderful staff at the STD/HIV clinic.
Pantibliss talking about being diagnosed with HIV in 1995. Managing death. Mixing the hemophiliacs, the gays, and the drug addicts #dotMED16
There was a lunch break and that we were back to the conference. We started with the dulcet sounds of Colm Mac Con Iomaire. It was amazing and let’s face it not many medical conferences can boast a session highlighted by a 300 year old Irish love song.
Colm was a founding member of the Frames, described to me by Suzanne Donnelly as Ireland’s greatest band not named U2.
Following Colm, they announced that PMD won the pitch session and then we were off with Deborah Bowman on Staging Medicine, or an actors perspective on the doctor-patient relationship. She talked about how medicine and theater are related. Her talk was filled with soliloquies taken from the stage.
Much of early practice in medicine is rehearsal to deal with realities without becoming an automaton: @deborahbowman#dotmed16
Following Deborah, was Ian Williams (@theBadDoctor). Ian is a comic artist and GP. He wrote a graphic novel, which he describes as a comic that requires a book mark. After he wrote the book he noted an explosion of medically themed graphic novels so he started a website to track and discuss them, Graphic Medicine. This website has made the cover of the BMJ and now has a yearly conference. He talked a bit about the history of drawing in medicine. It has until very recently been dominated by the illustrations of other peoples disease. Today we are seeing artists drwing there own illnesses.
I am happy to say that we now own a print of this image. Our souvenir from #dotMED16.
He tells the funny story that he put a barcode in a comic in the Guardian. The barcode resolved as a pretty rude statement. He thought it would take a few weeks to be discovered. The very first comment on the comic spilled the beans.
Early in his talk he recounted how he was given advice to begin his novel with lots of humor to engage his audience and leave a lot of the punch to the end. Which is exactly how he structured his talk at dotMED.
#dotMED16 when he started to write House of God he was told it needed to ride on humor. But the last third gets really dark.
He started with a charming story about how during medical school he did his OB rotation in Dublin at Hollis Street. He said it was the drunkest period of his life. He says he and his buds would get hammered at a pub then stumble back into OB ward and deliver a couple of kids. The nurses would only give him the easy ones, the moms that were delivering kid number 20. The audience was laughing uncontrollably but looking back it is kind of a horrifying story. Just like the House of God, I guess.
He told the story of how he got House of God published. He wrote the first 50 pages and he sent it off to an agent. He didn’t know what he was doing and the drat was single spaced and filled with typos and notes in the margin. A few weeks later he had forgotten all about it and received a call from the agent saying he was either insane or a genius. Later on the publisher asked if anyone in the book was identifiable. Stephen thought, “everybody” but answered just one, the chief of medicine, a renologist, who tucked his stethoscope into his pants. Son the lawyers gave him a large birthmark on his face to vaccinate them from a lawsuit.
He talked about the most important thing in medicine is connecting with a patient.
#dotMED16 how do you teach students how to deliver bad news. Do what the Fat Man does.
He elaborated on the healing power of connection by talking about his own alcoholism. He in recovery and a believer in alcoholics anonymous. He wrote a play about the origin of AA called Bill W. and Dr. Bob and explained that the core truth about AA is about connection:
#dotMED16 The only thing that can keep a drunk sober is telling his story to another drunk. The treatment is connection.
After his talk, Muiris interviewed him. Muiris started by mentioning that peope are always warned against meeting their heroes but meeting his hero, Stephen Bergman, has been wonderful.
Following the interview there was a wine and appetizers mixer. It was great to get a chance to chat with everybody at the conference. One of the remarkable things about dotMED was just how interesting everyone in attendance was. It was great chatting with them.
Then we went off for one last dinner and finally wrapped up up dotMED at Dex.





























{kind=link}