

UPDATE: please see this post with newer, more definitive data.
Initial patient visits for autosomal dominant polycystic kidney disease are different from just about any other patient visits. It is the only disease in which I spend a significant amount of time discussing the areas of bleeding edge research that have promise but are not yet available. I tell my patients about three current research thrusts:
- Combination ACEi-ARB
- ADH-antagonists
- mTOR inhibitors

{kind=link}
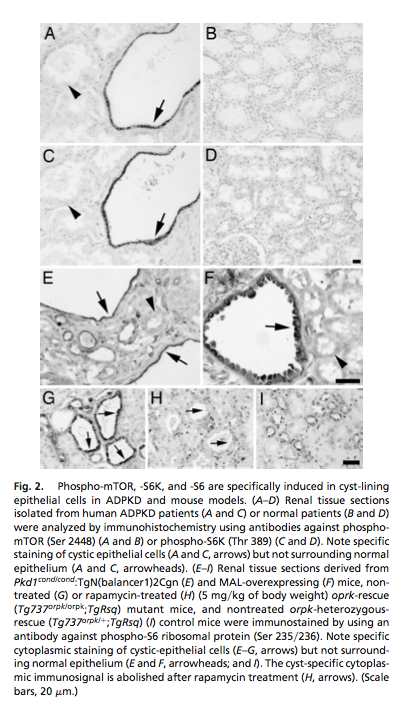
 Polycystic kidney disease cells show abnormal activation of the Ser/Thr kinase target of of rapamycin. This enzyme coordinates cell growth and proliferation. In three animal models of PKD, there is evidence of inappropriate activation of mTOR in the renal cysts. Because of this, blocking mTOR with rapamycin (same thing as sirolimus) is one of the most promising research avenues in ADPKD.
Polycystic kidney disease cells show abnormal activation of the Ser/Thr kinase target of of rapamycin. This enzyme coordinates cell growth and proliferation. In three animal models of PKD, there is evidence of inappropriate activation of mTOR in the renal cysts. Because of this, blocking mTOR with rapamycin (same thing as sirolimus) is one of the most promising research avenues in ADPKD. In this latest study by Perica et al. they had 21 patients and they received either conventional therapy or sirolimus (initial dose: 3 mg daily) for six months and then each patient crossed over to the opposite arm, so every patient received both control and experimental therapy. Six patients dropped out for various reasons and the researchers ultimatly reduced their target sirolimus levels from 10-15 ng/ml to 5-10 ng/ml. The authors explained the adverse reactions in the discussion:
Three patients were prematurely withdrawn from the study because of the onset of an erythema nodosus in one case and thrombocytopenia in two cases after a few days of sirolimus therapy, when sirolimus dosage was titrated to target trough levels between 10 and 15 ng/ml (all events fully resolved with treatment withdrawal). The poor tolerability of this high-dosage regimen led us to reduce the target levels to 5 to 10 ng/ml. With this approach, no serious event requiring treatment interruption was observed.
The primary outcome was change in the kidney volume. The authors, additionally, looked at changes in cyst volume and renal parenchymal volume which was important as they found an increase in the renal parenchyma with stable cyst volume during sirolimus and a reduction in renal parenchyma and increase in cyst volume during usual care.
The primary outcome, a change in renal volume was not significant, P=0.45; however, cyst volume increased more on conventional therapy, P=0.013 and parenchymal volume increased more on sirolimus, P=0.005.

Hypercholesterolemia is another widely known adverse effect of mTOR inhibitors. Our data, however, show that in patients without concomitant medications that may also ad- versely affect the lipid profile, such as steroids or calcineurin inhibitors, hypercholesterolemia is mild and can be easily managed just with dietary counseling. Thus, this adverse effect does not seem to be a major drawback of sirolimus therapy, even in the case of prolonged exposure.
Great article. Thanks, doctor, for the encouraging news!