One night that I was on call, I received an interesting patient from the ED.
The patient was confused but walked into the ER and was able to give at least a partial history. They did some initial chemistries and called me with the following results:
This is the kind of lab that grabs your attention.
With that glucose the first thought should be, “Is this DKA?”
Yes.
Beta-hydroxybutyrate: 6 mmol/L
I try to account for the anion gap. So I look at all the anions I measure and see how well they explain the gap. And if I can’t account for the majority of the gap I have difficulty sleeping. This patient’s gap was 51, 12 is normal which leaves 39 to account for. Only 6 can be accounted for with beta-hydroxybutyrate.
“Is there a lactic acidosis?”
Yes.
Lactate:16
That still leaves 17 mmol/L of unexplained anions.
Propylene glycol is normally due to the solvents used to dissolve IV drips. So usually we see problems in patients who have been in the ICU for awhile.
Propylene glycol is also found in antifreeze and hydraulic fluids.
The molecular weight is 76, so the 8.1 mg/dl represents only about 1 mmol/L, however it may explain the severe lactic acidosis and by stimulating the production of D-lactate it may explain even more of the gap.
Dialysis removes the parent compound and metabolites. Whether patients need to receive fomepizole is less clear. Kraut and Kurtz suggest fomepizole would be beneficial, while others feel less strongly.
Fomepizole not needed in PG toxicity. IMO, propofol, PG, & paracetamol (APAP) should replace phenformin in MUDPILES. https://t.co/B3PTX2cjOc
This question came in after class from a couple of students.
If the urine sodium in volume depletion and the great edematous states (heart failure, liver failure, and nephrotic syndrome) is low how can the urine osmolality be high?
The osmolality of the urine is made up of electrolytes (sodium, potassium and chloride) and non-electrolytes. The non-electrolytes like urea and ammonia will make up the bulk of the osmolality in the small volume of urine that is seen in this clinical setting.
In the advanced electrolyte class (nephrology and critical are fellowship) we look at the electrolyte content of the urine and use it to look at hypo- and hypernatremia more sophistically. For the purpose of medical school, SHELF exams, and USMLE parts 1, 2, 3 you can safely just look at the osmolality of the urine. We are trying to build a model that is understandable and good enough to predict how patients will behave in health and illness. This works pretty good.
The next question also came from a couple of people in class.
In SIADH, you say that the patients are euvolemic, but then you say they retain water via ADH in the medullary collecting duct. How can both of these be true? Won’t they become volume overloaded if they retain water.
This is a common question. The key to understanding this takes a bit of a leap of faith. First off, there is no slight-of-hand here. If you do careful water measurements as patients develop SIADH you can measure an increase in total body water. But critically, the increase in water is not progressive and it does not cause clinically significant volume overload. It does not cause pulmonary edema, it does not cause peripheral edema and it does not cause hypertension, all consequences of true volume overload from a positive sodium balance.
One of the reasons that excessive water intake does not cause volume overload is that most of that water (two-thirds) disappears into the intracellular compartment. Just like no one complains of their rings not fitting after drinking a lot of water, having high ADH does not cause interstitial edema.
This image from the lecture needs to be front and center when you think about SIADH: water out of balance, sodium in balance:
The last question for now comes from an e-mail (jtopf@mac.com):
I had a question from the second half of the lecture about treating euvolemic hyponatremia in the case of adrenal insufficiency. I’m having a hard time understanding why urea and salt tablets would help to reverse the hyponatremia. If solute in = solute out and the kidneys are already in sodium balance, how would it increase the solute load in the case of salt tablets? Even if the urine output goes up, won’t there still be non-physiological ADH release and concentration of the urine?
So the best way to think about salt and urea tablets is be visualizing this slide from this SIADH lecture:
In SIADH, the secretion of ADH is fixed and maximal. It’s like somone is stepping on the gas and can’t remove his foot.
Normally the ADH slides from minimal to maximal in order to balance water excretion with variable water intake:
The ADH slider is supposed to indicate that the ADH can slide from minimal activity, resulting in large volumes of urine, to maximal activity, resulting in minimal urine output. As the questioner correctly intuited, the osmolar load is fully excreted. In euvolemic hyponatremia, the slider is jammed to the right. If the urine osmolality (the denominator) is fixed the only way to adjust the urine volume will be to adjust the osmolar load (the numerator). Increasing the osmolar load with a high protein diet or salt tablets or urea pills will raise the numerator and hence increase the urine volume. It’s just math. Yes, taking sodium tablets will just result increase the sodium excretion since these patients are in sodium balance, but this additional sodium excretion increases the urine output making it easier for the patient to have less water intake than excretion, the goal for the treatment of hyponatremia.
Here is a link to the resources I used last year. They are largely unchanged. The water and solute lecture is available under the lecture tab. I will continue to edit this post with additional materials and links.
PBFluids has been quiet. Took awhile to just clear the cobwebs to get this post up.
One of the things that has kept me busy has been a project with a company called MedMastery. Franz Wiesbauer was a fan of my fluids book and reached out to me. We worked together to create a curriculum covering body water, diuretics, IV Fluids, sodium and potassium. The full course is about 1,000 slides. But the genius of MedMastery is how they edit and craft the course so it is broken up into an odd fifty 6-minute morsels. It is medical school for Generation Keurig.
MedMastery has opened up a few of the K-cups for promotion.
Art Levinson is the current Chairman of Apple. He was brought on to the board in 2000 during Job’s second act and was present for the introduction of the iPod, iTunes and iPhone.
Art Levinson is always introduced as the former CEO of Genentech but I didn’t know his story until I read the Herceptin story in Emperor of All Maladies. Turns out Levinson was trained by Nobel Michael Bishop of oncogene fame. In the late 80’s Levinson was leading a group pursuing treatment for breast cancer by doggedly tracking a gene called HER-2. Genentech’s executives turned away from cancer research after some high profile failures in the 80’s. This should have been the end of genentech’s role in HER-2 except for the leadership of Levinson. He dodged the bureaucracy, pursued resources and lead a small team to continue work on HER-2. The group produced Herceptin, one of the most important breakthroughs in chemotherapy in the molecular era in, a jaw-dropping, 3 years. Laureate
Reading that story I can see why Jobs would want him on the Apple board.
As we were gearing up for NephMadness Mealnie Hoenig mentioned that she loved working with the Nephmadness crew because they were “her people.” This resonated with me and has become my latest way of looking at the word. This particularly resonated with me when my college roommate introduced me to Public Broadcast Service.
Gene Kranz
There best song is “Go” which samples Gene Kranz dialog with his flight controllers during the Apollo 11 lunar lander landing. I love this because though I have heard the story of the Apollo mission a 100 times I had never thought of it from the perspective of the flight controllers.
This struck me as a great example of my people. While I never could imagine myself as Neil Armstrong, I could imagine me, and my ilk, being a flight controller in Houston. Which one would I be? flight SURGEON, of course.
Summary of the different flight controllers can be found here.
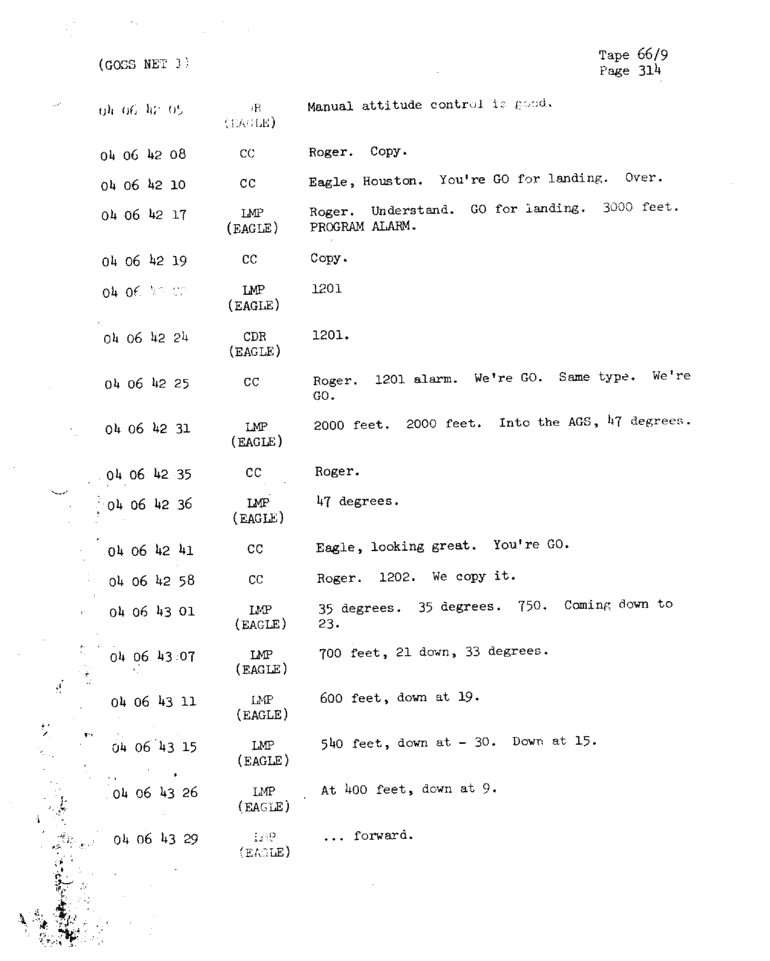
Transcript from the song:
Narrator (NASA Spokesman?) This is Apollo Control 102 hours into the flight of Apollo 11. It has grown quite quiet here at Mission Control A few moments ago Flight Director Gene Krantz requested that everyone sitdown and get prepared for the events that were coming and he closed with the remark “Good luck to all of you.” [Ed. not quite One small step for man; one giant leap for Mankind] 12 minutes now until ignition for powered descent. Everything still looking very good at this point Gene Krantz Okay all flight controllers, “Go” “No go” for powered descent.
CAPCOM we are go for powered descent [CAPCOM, capsule communicator, was an astronaut in Houston responsible for communicating with the mission astronauts. At the time of the landing it was Charlie Duke] We are off to a good start. Play it cool. Okay all flight controllers, I’m going around the horn RETRO? Go! FIDO? Go! GUIDANCE? Go! CONTROL? Go! Deltcom? Go! GNC? Go! EECOM? Go! SURGEON? Go!
Armstrong: Houston…ah…Tranquility base here. The Eagle has Landed.
Kranz: Okay keep the chatter down in this room. [The greatest moment in the history NASA and Kranz is focused on keeping his team on task]
CAPCOM: T1 standby for T1
Kranz: Stay or no Stay all flight controllers [Apparently it was possible to land on the moon but have something go wrong requiring an immediate return to orbit, so this was a check to see if they could proceed to the lunar surface mission]
no need to determine stone composition prior to treating stones
no need to analyze blood chemistry before treating stones
no need to do 24-hour (or 48-hour) urine collections before treating stones
What makes those positions so absurd is that if increased fluid intake did not reduce stones the authors suggested a trial of allopurinol, thiazide diuretics or citrate (without guidance on how to dose, follow or how to choose among those therapies). These recommendations are based on research done on patients where the type of stone had been determined. Not following those enrollment criteria makes the conclusions irrelevant.
It is as if the ACP said not to measure blood pressure because there has never been a randomized controlled trial of patients where blood pressure was measured versus patients who do not measure blood pressure.
Goldfarb’s letter added some other incredible details to the story I was unaware of including:
None of the authors of the paper have a single other co-authorship in PubMed relevant to kidney stones, other than the AHRQ review. I believe that none of the authors are nephrologists or urologists, none have a kidney stone clinic, none appear at, or present research at, kidney stone meetings, none have any experience regarding management of kidney stones
And this doozy, in response to a comment of the paper from the lead author:
As we point out in the guideline, we are aware that many physicians do select medications based on stone type, for example, allopurinol for uric acid stones, and we do not discourage that practice.
Physicians who regularly treat stones or who played NephMadness (2014 edition) know that allopurinol is used to prevent calcium stones not uric acid stones which are best treated with alkalinization.
Swapnil and I are delighted with the success of the endeavor which launched with humble beginnings on Medium aweek before the first chat with this manifesto:
Coincidental to the calendar turning over, NephJC is being recognized in two articles in the medical literature. The first is the first systematic review of microblogging journal clubs. It is an interesting and thought provoking article. NephJC takes a victory lap in Table 2:
NephJC is third in participants and total number of tweets and first in tweets and impressions per month. I found this paragraph particularly insightful: